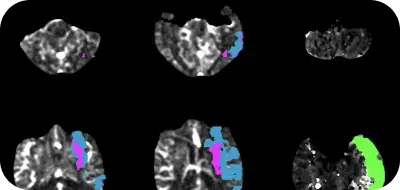
The Alberta Stroke Program Early CT Score (ASPECTS) is essential for clinical decision-making when treating ischemic stroke patients. It helps measure early ischemic changes and predict the functional outcome of endovascular thrombectomy.
ASPECTS is determined by evaluating 10 pre-defined regions of the middle cerebral artery vascular territory for focal hypoattenuation; however, studies have reported considerable variability in interrater agreements for ASPECTS, and the accuracy may depend on the reader's experience levels.
Diagnostic accuracy plays a crucial role in stroke triage and treatment decisions. Adding Rapid ASPECTS to the clinical workflow can assist non-neuroradiologists (and neuroradiologists) in evaluating NCCT scans and improving reading accuracy. For example, emergency physicians are often the first to evaluate and treat patients with an acute stroke given not all emergency departments have immediate access to expert stroke neuroradiologists.
According to a recently published retrospective study by Dr. Lambert and co-authors, the availability of automated ASPECT scores by Rapid ASPECTS when evaluating baseline non-contrast CT scans of patients with acute ischemic stroke resulted in a more uniform and accurate ASPECT scoring.
Key takeaways:
- The agreement of ASPECT scores for all test readers individually versus the criterion standard improved with software assistance, as did the interrater agreement.
- ASPECTS accuracy (or area under the curve) improved with the assistance of the automated software from 0.72 to 0.82 (P < .004).
174 patients with occlusions in the anterior circulation and whose baseline NCCT scans were available were included in the study. These patients were admitted to the University Hospitals Leuven (Belgium) between 2015 and 2018 and underwent thrombectomy for acute ischemic stroke.
Two experienced neuroradiologists reviewed the NCCT scans separately and set the criterion standard.
The test readers included a radiology resident, a stroke neurologist, a neurology resident, and two radiologists interested in neuroradiology. All raters scored ASPECTS in both hemispheres, blinded to clinical information and follow-up imaging.
Rapid ASPECTS evaluated all the scans and provided automated ASPECTS scores.
Several weeks after the initial scoring, the test readers were given the same scans, their previous scores, and the automated ASPECT scores. They could re-evaluate their scores now with additional information from the automated software.
With Rapid ASPECTS assistance, the accuracy and uniformity of ASPECT scores improved.
The test readers' agreement with the criterion standard varied from fair to good. The weighted Cohen kappa score (k) ranged between 0.38 and 0.76.
The agreement with the criterion standard was moderate (weighted k = 0.59) for the automated ASPECTS.
The agreement for all test readers individually versus the criterion standard improved with software assistance, as did the interrater agreement (overall Fleiss k = 0.15–0.23; P < .001).
Overall, the accuracy (or area under the curve) improved with the assistance of the automated software from 0.72 to 0.82 (P < .004).
The findings from the retrospective study by Dr. Lambert and co-authors suggest that Rapid ASPECTS' assistance when reading NCCTs of patients with acute stroke will result in a more uniform and accurate ASPECTS scoring.
Rapid ASPECTS is the only automated ASPECTS software to receive CADx clearance from the FDA.