A prospective pilot study showed that Rapid for Angio’s analysis of cone-beam CT perfusion (CBCTP) data delivers results comparable to that of Rapid CTP’s analysis of multidetector computed tomography (MDCTP) data in large vessel occlusion patients. Rapid for Angio could therefore aid in selecting patients eligible for endovascular treatment (EVT).
The findings by Dr. Darko Quispe-Orozco were published in Stroke.Key takeaways:
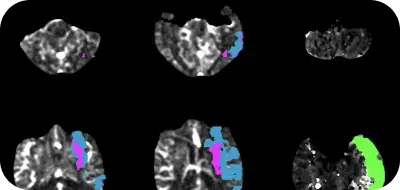
- RapidAI software’s estimation of ischemic core and hypoperfused tissue volumes on CBCTP and MDCTP are comparable
- Taking suspected ischemic stroke patients directly to an angio suite can help decrease stroke treatment time.
CT perfusion in the angio suite can help reduce workflow times and improve patient outcomes
An angio suite is a fully equipped space where a patient can undergo pre-operative care, the procedure, and post-operative recovery. Dedicated state-of-the-art angio suites can make a positive impact for conditions like stroke, where time plays a critical role in improving outcomes.
Since patients are frequently re-imaged just before their EVT to confirm that they are suitable candidates for the procedure, re-imaging these patients in the angio suite can come in handy and save time. Thrombectomy-enabled comprehensive stroke centers are beginning to directly admit their transferred and suspected LVO late-window patients to the angio suite, bypassing emergency department admission to save time.
The benefits of Rapid CTP’s analysis of MDCTP data to select patients eligible for EVT have been validated in multiple clinical trials. This pilot study evaluated whether Rapid for Angio’s analysis of CBCTP data can yield similar results.
Rapid for Angio is optimized to analyze CBCTP data and is now globally available with the Siemens Healthineers ARTIS icono.
Rapid for Angio’s analysis of CBCTP data was comparable to Rapid CTP’s analysis of MDCTP data
This interventional pilot study included 13 patients who were eligible for EVT and diagnosed with anterior circular LVO. The patients underwent CBCTP followed by MDCTP. To ensure that the perfusion conditions were similar, the time between the two imaging procedures was kept short and a low dose of contrast was administered prior to MDCTP. Rapid software was used to process and analyze both MDCTP and CBCTP data.
To determine the ischemic core volume, cerebral blood flow (CBF) of <30% (in comparison with the contralateral side) was set as the threshold on MDCTP. CBF of <45% was set as the threshold on CBCTP. Hypoperfused tissue volumes were evaluated at two thresholds, Tmax > 6s and Tmax > 10s.
There was a strong correlation between Rapid software’s estimated ischemic core and hypoperfused tissue volumes on CBCTP and MDCTP. The Bland-Altman analysis showed 92% agreement for the two parameters. The interclass coefficient of the estimated ischemic core volume was 0.89 (95% CI, 0.67-0.96) and the interclass coefficient of the estimated hypoperfused tissue volume (Tmax > 6s) was 0.86 (95% CI, 0.55-0.96).
In addition, there was a strong correlation between ischemic core volume estimated using CBCTP and the final infarct volume in patients who underwent reperfusion, with 90% agreement and 0.81 (95% CI, 0.48-0.94) interclass coefficient.
This pilot study provides evidence that Rapid for Angio optimized for CBCTP could be a helpful addition to facilitate stroke workflow and stroke care.