Neuroimaging has played a significant role in the stroke workflow following the DAWN and DEFUSE 3 trials and revised guidelines for acute ischemic stroke treatment. It helps determine which patients are eligible for endovascular thrombectomy (EVT) in the late window.
Demand for EVT transfers has increased, and the transfer of patients from community hospitals to Comprehensive Stroke Centers (CSCs) that can perform EVT has grown significantly in recent years. Not all transferred patients, however, undergo EVT, with the completion of infarct, clinical improvement, or interval recanalization being the primary reasons.
According to a retrospective study published by Dr. Mary McCullough-Hicks and co-authors, having a stroke physician at the CSC review the neuroimages before transfer significantly increases the likelihood of the patient undergoing EVT.
Not all referring hospitals have access to specialists on-site, and using software such as RapidAI to share patient imaging and clinical data with stroke physicians at the CSC can improve transfer decision-making.
Key takeaways:
- Patients whose imaging was available for review by a stroke physician at the CSC before transfer were significantly more likely to undergo EVT (68% vs. 54%, RR 1.26; p=0.006, 95% CI 1.09-1.48).
- When the stroke physician reviewed CT perfusion images via RapidAI software, the transferred patients were significantly more likely to undergo EVT (70% vs. 54%, RR 1.30; p=0.01, 1.09- 1.56).
Reviewing images before accepting patient transfer from a referring hospital - Stanford University Hospital
Margy McCullough-Hicks and co-authors hypothesized that 1) the availability of neuroimages for stroke physicians at the CSC to review before accepting a transfer will improve EVT eligibility and higher rates of EVT. 2) Performing certain types of imaging, regardless of availability for the CSC to review, increases the likelihood of EVT upon arrival.
A retrospective study analyzed a database of acute ischemic stroke patients diagnosed with large vessel occlusion and transferred from a primary stroke center to Stanford University Hospital (SUH) between 2015 and 2019 for EVT.
At SUH, a multidisciplinary team comprising a stroke fellow, stroke attending, and stroke interventional radiologist decide whether to accept a transfer request from a referring hospital based on clinical presentation and neuroimages (when available).
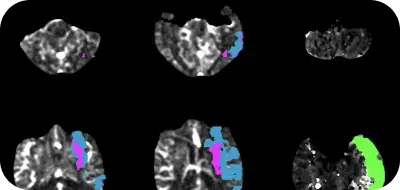
RapidAI is one of the options available to SUH to examine scans of patients at the referring hospital before accepting a transfer. SUH also uses Telestroke and LifeImage to share clinical and imaging data between hospitals.
A total of 525 patients who were transferred from referring hospitals to SUH between 2015 and 2019, with concern for acute LVO stroke and with the intent to treat with EVT, were included in the analysis. 268 patients underwent EVT (50.8%). 147 (28% of the total) had pre-transfer neuroimaging available for the SUH team to review before transfer acceptance.
RapidAI software supports shared decision-making before transferring patients from a referring hospital to a CSC.
Patients whose imaging was available for review by a stroke physician at the CSC before transfer were significantly more likely to undergo EVT (68% vs. 54%, RR 1.26; p=0.006, 95% CI 1.09-1.48).
When the stroke physician reviewed CT perfusion images via RapidAI software, the transferred patients were significantly more likely to undergo EVT (70% vs. 54%, RR 1.30; p=0.01, 1.09- 1.56).
Patients who received EVT were more likely to have had pretransfer vessel imaging, regardless of whether it was reviewed by a specialist at the CSC (76% vs. 59%, RR 1.44; p<0.001, 1.18-1.76).
Reducing futile transfers becomes essential, given the limited resources in CSCs and the costs involved in patient transfers. Patient transfers are more effective when stroke teams at the CSCs and referring hospitals are connected with AI-powered imaging data.
Rapid CTP is the only FDA-cleared software to aid patient selection for acute stroke therapy.