



Clinical evidence
Results strong enough to rewrite guidelines

The strongest clinical history, fueling results you can count on
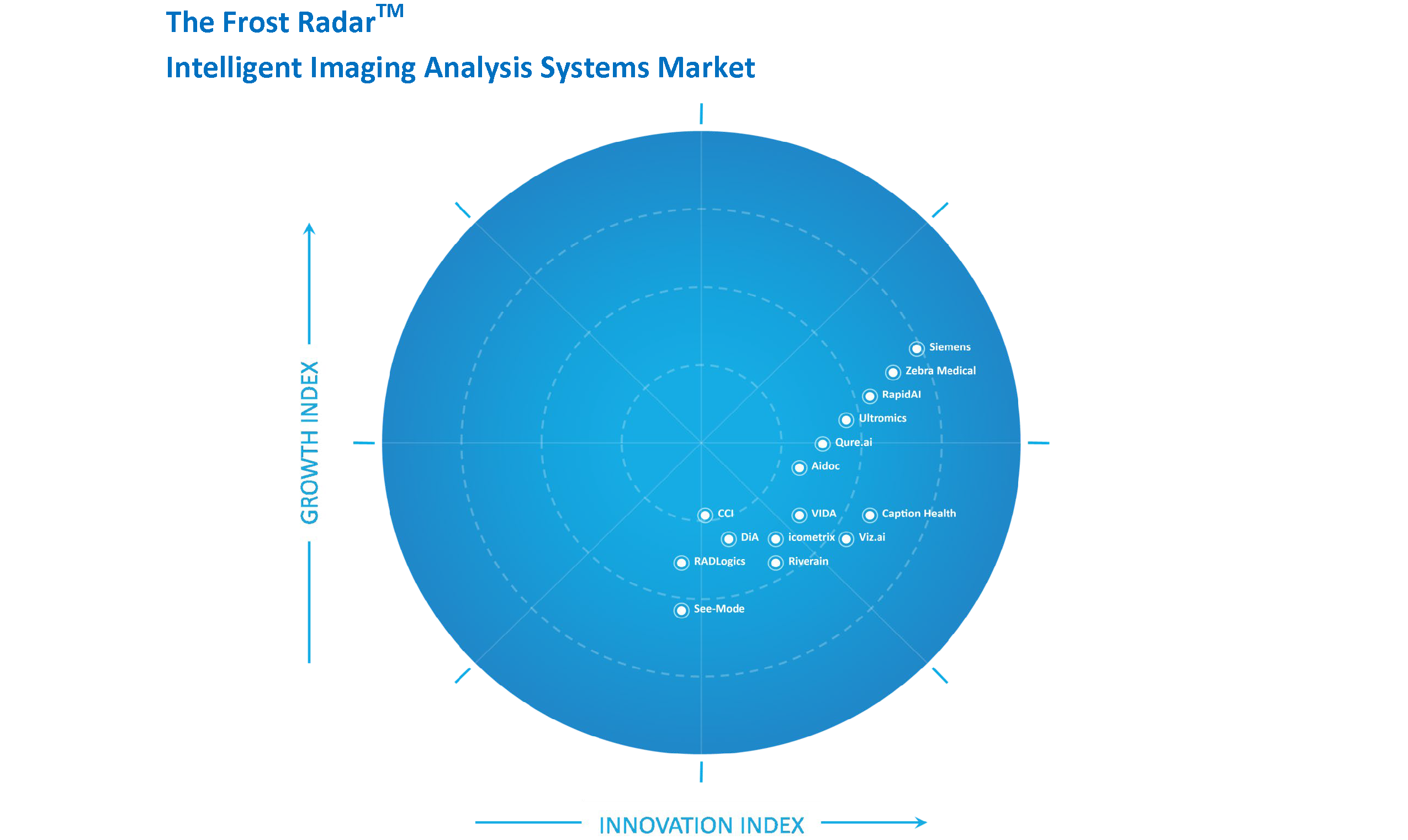
Used in the most influential stroke trials around the world, Rapid-based trials have achieved world-class results in endovascular stroke studies. But the influence doesn’t stop there.
25+
Clinical trials
1,000+
Clinical studies
750+
Publications
11
NEJM publications
17.5
AVG impact factor
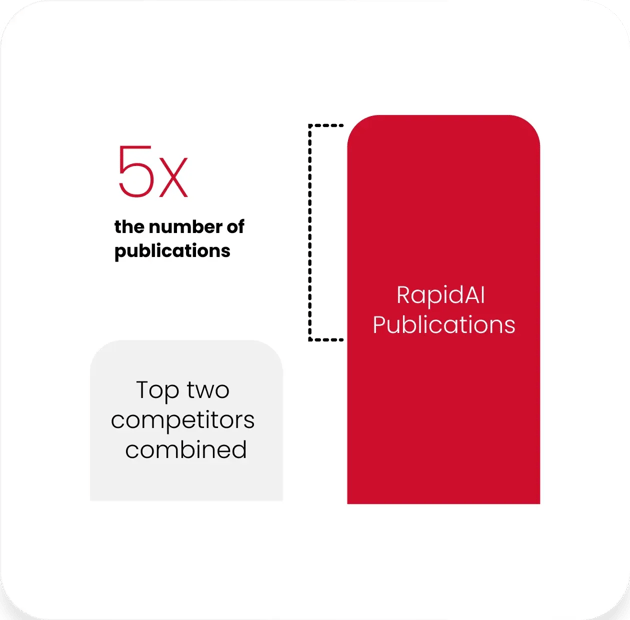
Clinical validation powers accuracy and the deepest AI-driven insights on the market.
Rapid has 5x the number of publications than our top two competitors combined.
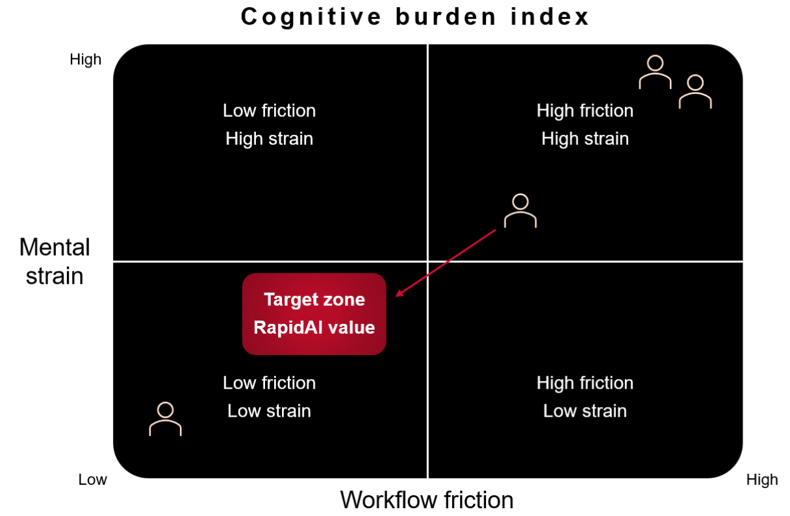
Game-changing technology, helping you push the limits
But really…these Rapid-supported trials changed AHA stroke guidelines – expanding the stroke treatment window up to 24 hours from symptom onset.
Swift-Prime
Demonstrated the value of mechanical thrombectomy in improving outcomes for large-vessel occlusions treated within six hours
Swift-Prime
Second highest rate of favorable clinical outcome in any endovascular stroke trial
EXTEND-IA
Showed advanced imaging selection, newer generation devices, and earlier intervention improves outcomes in 0-6 hr windows
EXTEND-IA
Highest rate of favorable clinical outcome (71%) in any endovascular stroke trial
DEFUSE 3
Early termination for efficacy of extended window (6-16 hrs) thrombectomy in carefully selected patients
DEFUSE 3
The first trial to demonstrate slower growth core infarct beyond 6 hrs
DAWN
Demonstrated superior outcomes using thrombectomy plus CMM vs CMM alone in 6-24 hr window
DAWN
Highest rate of clinical benefit in any endovascular stroke trial. 36% absolute risk reduction

Ongoing pursuit to push the boundaries of care
Our commitment to staying at the forefront of clinical innovation is as strong today as it was a decade ago.